
Locator Fixed™
Case Report A New Way to Deliver Fixed Full-Arch Restorations Utilizing Traditional Locator Abutments & A New Fixed Attachment System
Case Report A New Way to Deliver Fixed Full-Arch Restorations Utilizing Traditional Locator Abutments & A New Fixed Attachment System
 Xavier E. Saab DDS, MS
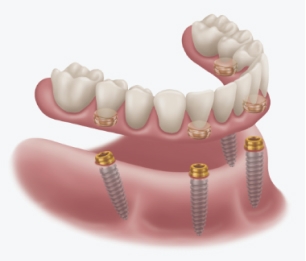
Xavier E. Saab DDS, MSThis article presents a new, innovative, and simple technique to deliver fixed full-arch prostheses utilizing a proven and well-known removable overdenture abutment (Zest LOCATOR). The new FDA approved fixed inserts (LOCATOR FIXED Attachment System) are designed to also work with standard LOCATOR abutments and leverage traditional denture fabrication procedures.
Introduction
The treatment of edentulous arches with fullarch fixed dental prosthetics is the oldest form of restorations placed on root form endosseous implants as presented by Branemark et al. in 1977. Many different techniques and philosophies of fixed full-arch restorations have been developed and described in the last 55 years which include but are not limited to different type of restorative materials, implant numbers and angulations, management of the restorative space, healing protocols, and analog or digital workflows. Even though some these variations of full arch therapy may be clinically simpler to perform than others, the final prostheses usually require final insertion with prosthetic screws than make the prosthetic material easier to fracture and create the necessity to utilize materials to seal screw access holes. These issues increase the maintenance times and the potential for prosthetic complications throughout the life of the prostheses. Imagine being able to design and build an FP-3 full-arch (fixed-detachable hybrid) prosthesis, utilizing the current techniques used to make a simple denture or overdenture. Imagine being able to deliver these prostheses with a single snap, and perform maintenance and repair appointments without having to drill screw access covers, removing screws, choosing new screws, and torquing the prosthesis, and resealing it after the required procedure.
Patient Background
Our patient presented with maxillary and mandibular terminal dentitions. Different options were discussed with him for the replacement of his teeth, which included complete dentures, implant-retained overdentures, and fixed prostheses on implants. After considering the costs and benefits of each alternative, the patient decided to have all his remaining teeth removed and replaced with maxillary and mandibular implant-retained overdentures.

Initial Treatment Plan
Interim dentures were fabricated prior to the extractions. All remaining teeth were removed, alveoloplasty performed, and implants placed at the same appointment. The interim dentures were inserted immediately after surgery with a tissue conditioning reline material. The patient was allowed to heal for 4 months, then the implants were successfully tested for osseointegration. LOCATOR abutments were selected and torqued as recommended by the manufacturer prior to beginning the definitive prosthetic treatment. Maxillary and mandibular implant-retained overdentures were fabricated using traditional indirect techniques. Both prostheses included metal frameworks for strength and long-term survival, and the LOCATOR housing were pickedup chairside at the time of delivery. Our patient reported to be very happy and pleased with his new smile at the time of delivery. But after several adjustment appointments he reported constant problems with his maxillary overdenture causing gagging and nausea after 1 or 2 hours of wearing his prosthesis. For over 1 year he only wore his denture a few hours per day and at mealtimes and he felt his quality of life had not improved since the time of extractions.
Revised Treatment Plan
We discussed the possibility of changing the type of prosthesis on the maxilla from removable to fixed. We explained to the patient the availability of a novel attachment system utilizing his existing LOCATOR abutments and he expressed being very excited about the possibility. A new maxillary complete denture was fabricated around the LOCATOR abutment utilizing the indirect technique and conventional procedures. This time the denture did not have a metal reinforcing framework, since it will be converted into a fixed prosthesis.

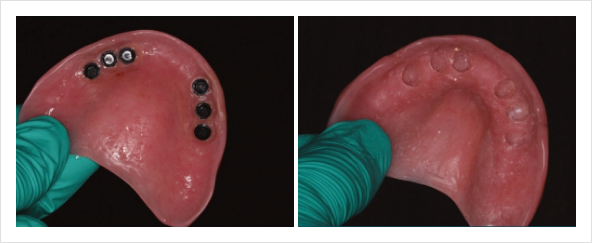
The day of delivery, new housings were picked up in the denture intraorally using CHAIRSIDE APM. Finally, the denture was converted in the laboratory by eliminating the palate, the flanges and all ridgelapping portions of the acrylic to create a welladapted, and hygienic fixed implant-supported prosthesis. No adjustments have been necessary since the insertion and the patient now reports much improvement in his quality of life without having to remove his denture, and with his gagging reflex resolved, he is now able to smile and eat without worrying about his teeth.
Summary

For over four decades the delivery of full-arch implant prosthetics has been a convoluted series of clinical and laboratory procedures that has made it challenging for the general practitioner to make this therapy easily accessible to a great number of patients in need. The use of the traditional LOCATOR abutment with the Fixed LOCATOR System, and simple removable prosthetic techniques will make full-arch implant rehabilitation a more predictable and economical way to reach many underserved patients. It will allow more general dentists to grow personally and professionally. And it will make the hygiene, maintenance, and repair appointments simpler and more efficient for the general dental practice.
800.262.2310
800.262.2310
800.262.2310